
Pearls for Internal Distraction Plating of Complex Distal Radius Fractures
Distal radius fractures are the most common type of fracture treated in emergency departments. According to Alexander H. Payatakes, MD, Penn State Bone and Joint Institute, “The vast majority of operative distal radius fractures can be successfully treated with a volar locking plate. However, standard volar locking plates don’t perform well when the fracture extends to the diaphysis or when there are grossly comminuted fragments too small to capture with screws. Adequate stability is especially important when the patient has also sustained lower extremity fractures that will require early loading of the wrist to ambulate with a walker or crutches.” Such fractures often occur in both older patients with osteopenia, as well as a result of motor vehicle accidents.
An alternative to external fixation for these types of complex fractures is an internal distraction plate. This involves a 3.5 millimeter LC-DCP plate or other dedicated dorsal bridging plate applied across the dorsum of the wrist through two or three small incisions in the forearm and hand (Figure 1).¹ The distraction plate is attached to the radius proximally and to either the second or third metacarpal distally (passing through the second or fourth extensor compartment, respectively). Payatakes adds, “Kirschner wires are typically used as an adjunct to further stabilize smaller fragments not reduced by the distraction plate.” (Figure 2) The advantages of an internal distraction plate over external fixation include: improved patient comfort, greater biomechanical stability allowing earlier weight bearing², no risk of pin track infection, and decreased risk of complex regional pain syndrome.
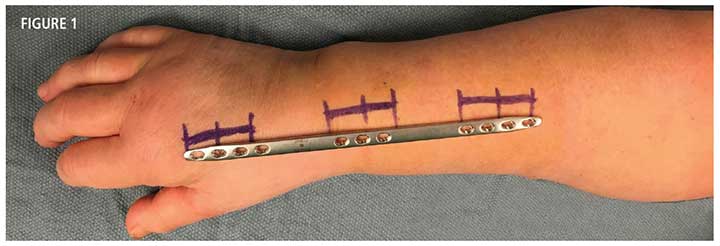
FIGURE 1: A 3.5 millimeter LC-DCP plate or other dedicated dorsal bridging plate to be applied across the dorsum of the wrist through two or three small incisions in the forearm and hand, attaching to the radius proximally and to either the second or third metacarpal distally.
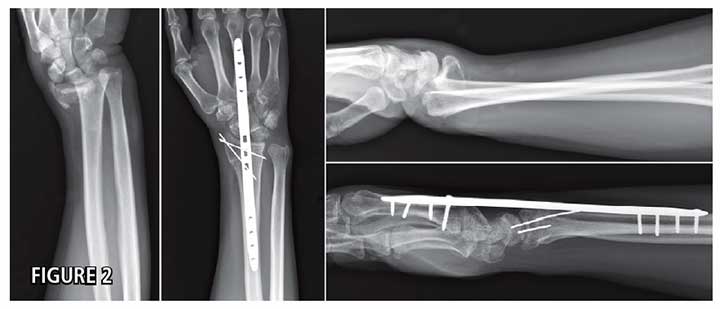
FIGURE 2: Kirschner wires are typically used as an adjunct to further stabilize smaller fragments not reduced by the distraction plate.
Payatakes notes several factors key to successful application of internal distraction plating. “When placing the internal distraction plate, it is very important to avoid entrapment of extensor tendons, which can lead to tendon attrition or even frank tendon rupture,” says Payatakes. A recent cadaveric study³ showed that tendon entrapment with the internal distraction plate is most likely to occur when the plate is attached to the third metacarpal, but can largely be avoided if attached instead to the second metacarpal. Payatakes also notes that over-distraction should be avoided at all costs, since it can lead to complications like digital stiffness and chronic pain.
“With over-distraction the tendons may be too tight, preventing normal range of motion. To avoid this, the radiocarpal joint space should remain smaller than 5 millimeters. After the plate is inserted, confirm full finger flexion, without any tightness. It is also important to confirm full passive forearm rotation before completing fixation,” he explains. The metal plate is not designed for long-term placement; Payatakes stresses the importance of its removal after the fracture has healed, typically after about three months’ time: “If the plate remains implanted for more than six months, it is highly likely to fail, with the additional risk of extensor tendon rupture.” The need to perform a second surgery for plate removal is a drawback of this approach, which must be considered when choosing the optimal solution for an individual patient.

Alexander Payatakes, MD
Orthopaedic Hand Surgeon
Associate Professor, Orthopaedic Hand Surgery
Phone: 717-531-5638
Email: apayatakes@pennstatehealth.psu.edu
Fellowship: Hand surgery, Duke University Medical Center, Durham, North Carolina, and Allegheny General Hospital, Pittsburgh, Pennsylvania
Residency: Orthopaedic surgery, University Hospital of Ioannina, Ioannina, Greece; Internship: General surgery, University of Patras, Patras, Greece
Medical School: University of Patras, Patras, Greece
Connect with Alexander Payatakes, MD, on Doximity
References
- Papadonikolakis A, Ruch D. 2005. Internal distraction plating of distal radius fractures. Tech Hand Upper Extrem Surg. 9(1):2-6.
- Wolf J, Weil W, Hanel D, Trumble T. 2006. A biomechanical comparison of an internal radiocarpal-spanning 2.4-mm locking plate and external fixation in a model of distal radius fractures. J Hand Surg Am. 31:1578-86.
- Lewis S, Mostofi A, Stevanovic M, Ghiassi A. 2015. Risk of tendon entrapment under a dorsal bridge plate in a distal radius fracture model. J Hand Surg Am. 40:500-4.
U.S. News & World Report 2025-2026
Penn State Bone and Joint Institute represents the clinical aspect of Penn State Orthopaedics and Rehabilitation. Faculty from Penn State Orthopaedics and Rehabilitation teach and perform leading-edge research in the department, and provide innovative care in the multi-disciplinary Penn State Bone and Joint Institute. As a department, Penn State Orthopaedics and Rehabilitation faculty, clinicians and researchers have been recognized nationally, ranking twentieth in orthopaedic research funding from the National Institutes of Health.
Continuing Education activities
Stay informed of all Continuing Education activities that interest you.